Kidney Ultrasound Images (POCUS): 4 Common Conditions and Scan Tips Using EagleView Portable Ultrasound
Kidney Ultrasound Images (POCUS): 4 Common Conditions and Scan Tips Using EagleView Portable Ultrasound
Written by Dr. Wiley (Pulmonology & Critical Care Physician) - Published on Jun 15, 2024
Sonography is an important method for diagnosing and treating kidney disease. This article summarizes the most common ultrasonographic findings for kidney disease for reference.
Kidney ultrasound is a core POCUS exam for bedside assessment of renal structure, collecting system changes, and perfusion. In this guide, we walk through ultrasound images and key scan tips for the 4 most common kidney conditions encountered in daily practice:
- Renal cysts (simple vs. complex)
- Hydronephrosis (collecting system dilation and severity cues)
- Chronic kidney disease (CKD) (cortical echogenicity, thinning, and atrophy patterns)
- Acute kidney injury (AKI) (what ultrasound can and can’t show, plus practical assessment points)
Before diving into these conditions, we start with what a normal kidney looks like on ultrasound. A clear “normal” baseline makes it easier to spot abnormalities quickly, describe findings consistently, and avoid common pitfalls during POCUS scanning.
Quick Takeaways (for fast reading)
Normal Kidney
Longitudinal scan with an ultrasound probe showed that the kidney was broad bean-shaped, and the right kidney was lower than the left kidney; the left kidney showed a single hump because it was close to the spleen. The kidney can be divided into the renal parenchyma and the renal sinus; the renal sinus is hyperechoic on ultrasound imaging and the renal parenchyma is hypoechoic: this can be divided into an outer cortical area and an inner medullary area (cone echo). Between the medulla is the renal column.
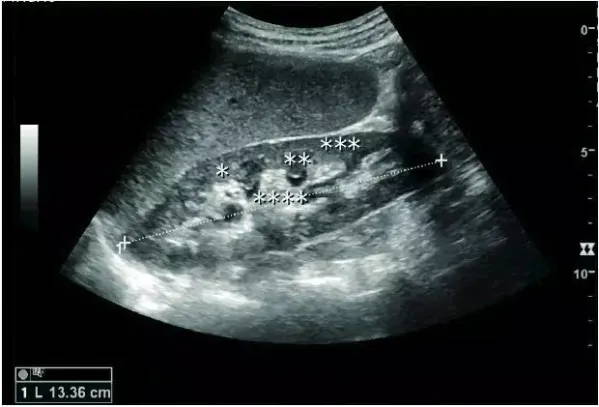
Normal adult kidney ultrasound scan image: *renal column, **renal pyramid, ***renal cortex, ****renal sinus
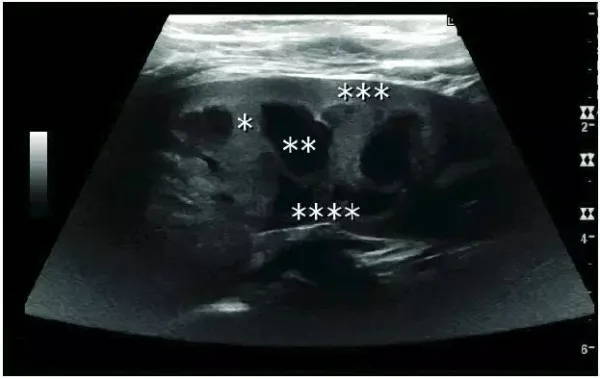
Normal child kidney ultrasound scan image: *renal column, **renal pyramid, ***renal cortex, ****renal sinus
The normal adult kidney is about 10-12 cm long, and the right kidney is slightly longer than the left kidney. Kidney size correlates with individual size and age. The renal cortical thickness is measured from the base of the renal vertebral body and is typically 7-10 mm. If the renal vertebral body is poorly demarcated, the thickness of the renal parenchyma can be measured and is 15-20 mm.
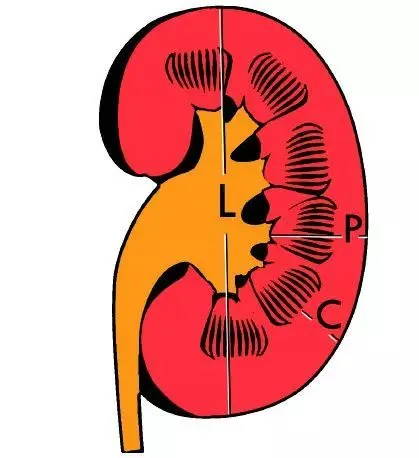
Renal measurements: L=length; P=parenchymal thickness; C=cortical thickness.
Renal Doppler ultrasonography is widely used in clinical practice and can accurately assess vascular perfusion. Spectral Doppler examination of renal arteries and interlobular arteries can evaluate peak renal artery systolic blood flow, resistance index and blood flow velocity curve, such as renal artery systolic peak blood flow ≥ 180 cm/s, which is renal artery stenosis ≥ 60. % predictors, resistance index ≥ 0.70 indicates abnormal renal vascular resistance.
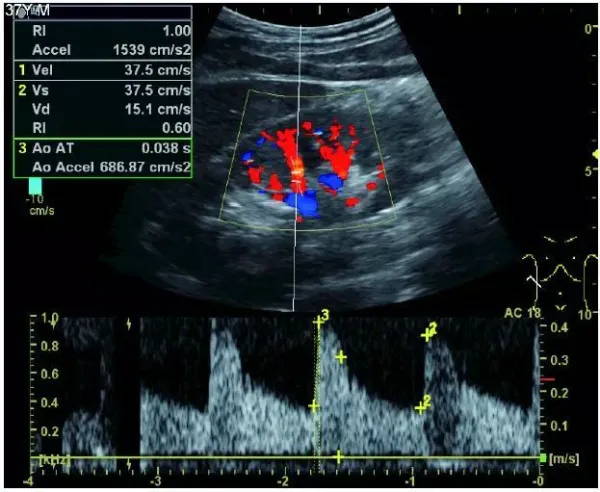
Doppler ultrasound image of a normal adult kidney. Red: blood flow into the transducer; blue: blood flow out of the transducer.
Renal Cyst
Most renal cysts are simple renal cysts that are round in shape and filled with fluid. The incidence of simple renal cysts in people over 50 years old is ≥50%. It is a benign lesion and no further evaluation is required.

Adult simple cyst, dashed distance: kidney length
Features of complex renal cysts: septation, calcification, and irregular thickening of the cyst wall. Doppler ultrasonography is feasible for further evaluation. Bosniak grading and follow-up of complex renal cysts can be performed with contrast-enhanced ultrasonography or enhanced CT. The Bosniak classification can be divided into grades I-IV, grade I: simple cyst, grade IV: cystic malignancy risk 85%–100%.
Adult complex renal cyst with wall thickening in the lower pole, +, dashed distance: kidney length and complex cyst
In patients with polycystic kidney disease, multiple cysts of varying sizes can be seen. In patients with advanced polycystic kidney disease, the kidneys are enlarged, with no obvious demarcation between cortex and medulla.

Advanced polycystic kidney disease with multiple renal cysts
Hydronephrosis
Renal ultrasonography is an important method for diagnosing and treating kidney diseases. The primary indication for renal ultrasound is to evaluate the renal collecting system. Dilation of the renal collecting system is often associated with obstruction of the urinary tract (including renal pelvis, calyces, and ureters). There is no echo in the hydronephrotic area, and renal sinus dilatation can be seen.
Hydronephrosis in children can be caused by obstruction of the ureteropelvic junction, ectopic ureteral orifice, primary megaureter, and posterior urethral valves (below). In adults, hydronephrosis can be caused by urolithiasis, obstruction of the renal pelvis or ureter, and ureteral compressions, such as pregnancy and retroperitoneal fibrosis. Urolithiasis is the most common cause of hydronephrosis in adults, with a prevalence of 10%-15%.

Hydronephrosis due to obstruction of the ureteropelvic junction in children
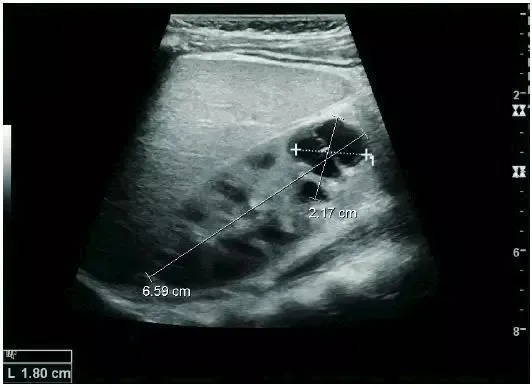
Hydronephrosis can be classified into five different grades from mild dilatation of the renal pelvis to thinning of the cortex based on macroscopic findings (Figure A). Hydronephrosis can also be assessed by measuring the level of the neck in the longitudinal section of the renal pelvis, the level of dilation in the transverse section, and cortical thickness (Figures B, C).

A: Late hydronephrosis with cortical thinning; +, dashed line distance: the dilated size of the renal pelvis

B: Renal pelvis, calyx dilation with cortical atrophy; +, dashed line distance: the width of the calyx in longitudinal section

C: Renal pelvis dilated size in transverse section
If abnormal echoes are seen in the collection system, clinical examination, blood analysis, and puncture or drainage should be performed to exclude pyonephrosis if necessary. Hydronephrosis can also be caused by non-obstructive diseases, such as taking diuretics, pregnant women, and children with vesicoureteral reflux.
Chronic Kidney Disease
Ultrasound is an important method for diagnosing chronic kidney disease and judging prognosis. Whether it is glomerulosclerosis, tubular atrophy, interstitial fibrosis, or inflammation, echogenic cortical enhancement is seen on ultrasound imaging. Normal kidney echoes are similar to those of the liver or spleen. In addition, renal atrophy and cortical thinning are common, especially as the disease progresses. However, kidney size correlates with height, and patients with short stature have smaller kidneys; therefore, kidney size should not be used as the sole criterion.

Chronic kidney disease due to glomerulonephritis: thinning of the cortex and increased echogenicity. +, dotted line: kidney length

Nephrotic syndrome: echogenic demarcation of renal cortex and medulla

Chronic pyelonephritis: renal atrophy, focal cortical thinning. +, dotted line: kidney length

End-stage renal disease: echogenic, homogeneous structure, inability to distinguish renal parenchyma from renal sinus with the naked eye. +, dotted line: kidney length
Acute Kidney Injury
Ultrasound is the method of choice for the detection of acute renal lesions; CT and magnetic resonance imaging (MRI) are options for evaluation when ultrasonography is difficult to detect. When evaluating acute renal lesions, renal echo, renal imaging, renal vascularity, renal size, and focal lesions should be observed.
Acute pyelonephritis: cortical echogenicity, ill-defined superior renal pole

Postoperative renal failure: increased cortical echo and enlarged kidneys. Kidney biopsy revealed acute tubular necrosis
CT is the method of choice for evaluating renal trauma, and ultrasound is used for follow-ups, especially in patients with suspected urethral tumors (see below).

Renal trauma: Infrarenal pole laceration, subcapsular effusion.
Ultrasound Guided Therapy
Kidney biopsy, percutaneous nephrostomy, or abscess drainage can be performed under ultrasound guidance. In the past, thermal ablation of renal tumors was guided by CT, because ultrasound-guided intervention was difficult to clearly display the intestinal distribution, resulting in a higher risk of peripheral intestinal injury. However, the latest guidelines for renal interventional therapy recommend ultrasound guidance as the preferred choice for radiofrequency, microwave, and cryoablation.
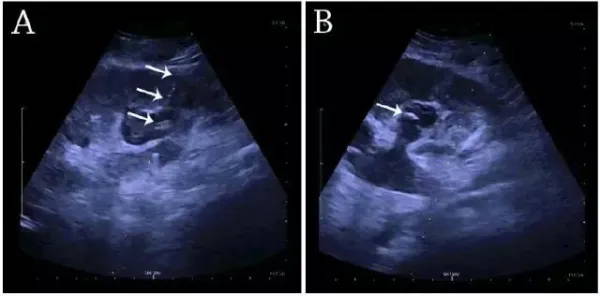
(A) Percutaneous nephrostomy with a fistula placed through the renal calyx into the hydronephrosis at the lower pole of the kidney. (B) Pigtail catheter placed in the calyceal dilatation. White arrows: fistula and pigtail catheter.
Percutaneous nephrostomy and abscess drainage can be performed using the one-step or Seldinger technique. Clinicians can choose one-step or Seldinger techniques based on preference, experience, and equipment conditions.
Conclusion
Renal ultrasonography is simple, convenient, rapid, and low-cost, and is an important method for diagnosing renal disease and guiding treatment. However, it still has certain limitations, and CT and MRI can be used to assist evaluation.
Related Products
Subscribe
Get promotions, ultrasound resources, case studies, and news here!
Point-of-Care Imaging in the Palm of Your Hand
3-In-1 Probe
No Subscription Fee
18/36-Month Warranty
30-Day Free Return
✔️ 30-Day Money-Back Guarantee